




菜单



立即预约

英 / 中



远程问诊

立即咨询




A note on terminology
This document uses tirzepatide to refer to the same generic compound, in line with Singapore's medical advertising guidelines, which restrict reference to registered trade names.
It's important to be clear about what is and isn't approved right now, so you can have an informed conversation with your doctor.
✓ 2022 — Approved for type 2 diabetes. Tirzepatide's first approval, internationally and in Singapore, was for blood sugar control in adults with type 2 diabetes.
✓ 2023 — Approved for weight management. Tirzepatide gained approval for chronic weight management in adults with obesity, or overweight with at least one weight-related condition, a category that can include sleep apnoea, high blood pressure, or high cholesterol. This is the approval currently in effect in Singapore.
✓ Dec 2024 — Dedicated OSA indication approved overseas. Regulators in the United States approved a specific indication for moderate-to-severe obstructive sleep apnea in adults with obesity, based on the SURMOUNT-OSA phase 3 trial results detailed below.
▸ Q3 (anticipated) — Dedicated OSA indication anticipated in Singapore. A dedicated sleep-apnea indication is anticipated to be approved by HSA around Q3. Until this takes effect, tirzepatide is not registered in Singapore specifically for the treatment of OSA on its own.
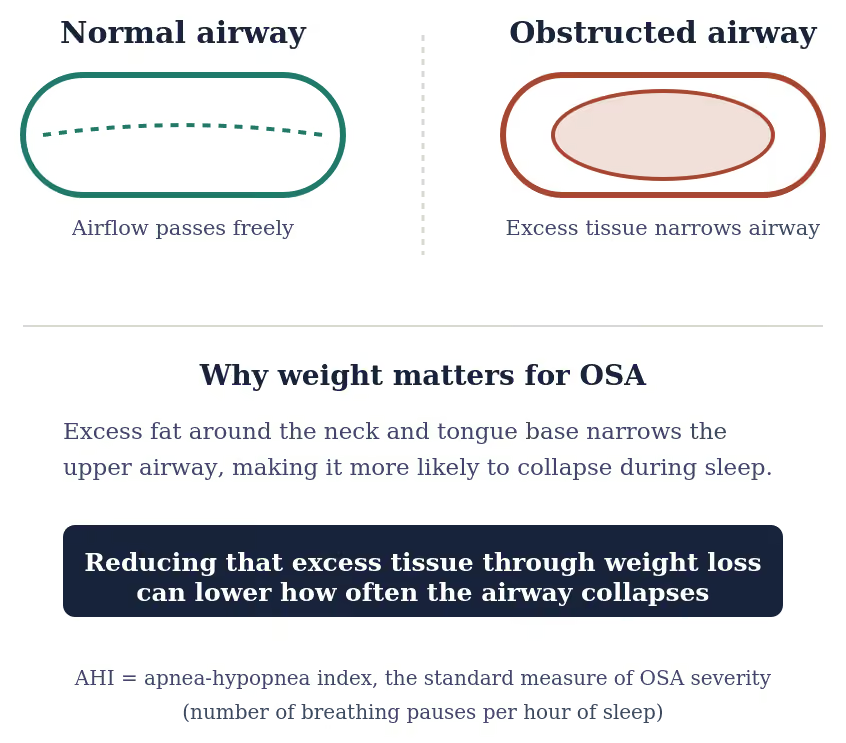
Obstructive sleep apnea is a common sleep-related breathing disorder in which the upper airway repeatedly collapses or narrows during sleep, causing pauses in breathing (apneas) or shallow breathing (hypopneas). It affects a very large share of adults worldwide and is closely linked to obesity, which is considered its most significant modifiable risk factor. (2)
Severity is measured using the apnea-hypopnea index (AHI), the number of breathing pauses per hour of sleep. Moderate to severe OSA is generally defined as an AHI of 15 or more events per hour. (3)
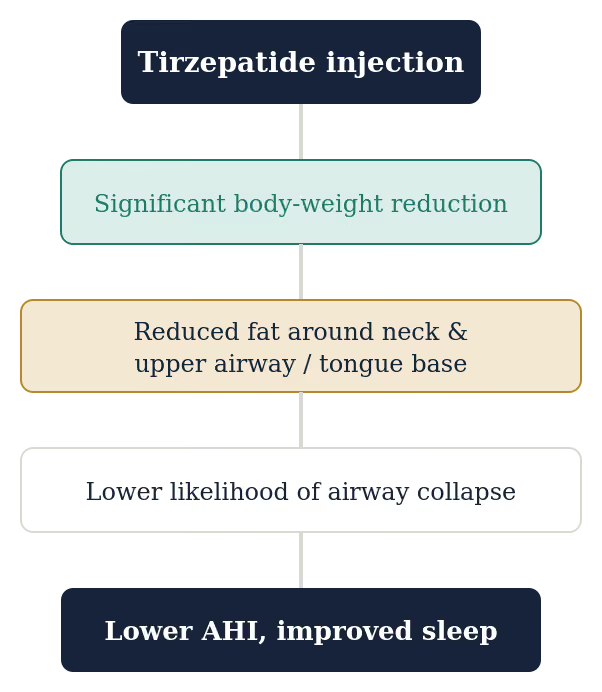
Excess fat deposited around the neck, tongue base, and upper airway narrows this passage and makes it more prone to collapse during sleep. Because of this mechanical link, treatments that produce substantial weight loss, like tirzepatide, have a plausible route to improving OSA severity, not just body weight.
SURMOUNT-OSA comprised two phase 3, randomized, double-blind, placebo-controlled trials in adults with moderate-to-severe OSA and obesity, run over 52 weeks. Study 1 enrolled participants not using positive airway pressure (PAP) therapy; Study 2 enrolled participants already on PAP therapy. (1) (4)
Study
Population (n)
AHI Result (events/hr)
AHI % Change from Baseline
Disease Resolution
Study 1
234 · no PAP therapy
-25.3/hr vs -5.3/hr placebo
55.0% vs 5.0% placebo
43.0% (highest dose)
Study 2
235 · on PAP therapy
-29.3/hr vs -5.5/hr placebo
62.8% vs 6.4% placebo
51.5% (highest dose)
At 52 weeks, AHI fell by a mean of 25.3 events per hour with tirzepatide versus 5.3 with placebo, an estimated treatment difference of 20.0 fewer events per hour. As a key secondary endpoint, this represented a mean 55.0% decrease in AHI from baseline in the tirzepatide group, compared with a 5.0% decrease from baseline in the placebo group. Mean body weight fell 18.1%, versus 1.3% with placebo. (1) (4)
At 52 weeks, AHI fell by a mean of 29.3 events per hour with tirzepatide versus 5.5 with placebo, an estimated treatment difference of 23.8 fewer events per hour. As a key secondary endpoint, this represented a mean 62.8% decrease in AHI from baseline in the tirzepatide group, compared with a 6.4% decrease from baseline in the placebo group, the largest such reduction across both studies. This figure is a change from each group's own starting point, not a direct comparison against placebo, so the events-per-hour treatment difference above is the more precise measure of tirzepatide's isolated effect. Tirzepatide also produced additional improvements in blood pressure and inflammatory markers. (1) (4)

Beyond AHI, the SURMOUNT-OSA trials measured several other outcomes. Tirzepatide significantly reduced:
However, the trial was not designed to prove that the improvement in OSA was independent of weight loss. (1)
Obesity contributes to OSA through more than excess body weight alone. It is also associated with chronic low grade systemic inflammation, upper airway inflammation, endothelial dysfunction, and altered respiratory physiology. They proposed that tirzepatide's benefits may extend beyond weight loss, potentially through improvements in these metabolic and inflammatory pathways. (1)
hs-CRP is a marker of systemic inflammation. In SURMOUNT-OSA, hs-CRP decreased significantly with tirzepatide, AHI improved substantially, and body weight decreased by approximately 18% to 20%. This raises the possibility that reduced inflammation may contribute to improved airway function or reduced disease severity. The study, however, was not designed to establish that the fall in hs-CRP caused the improvement in OSA. (1) (9)
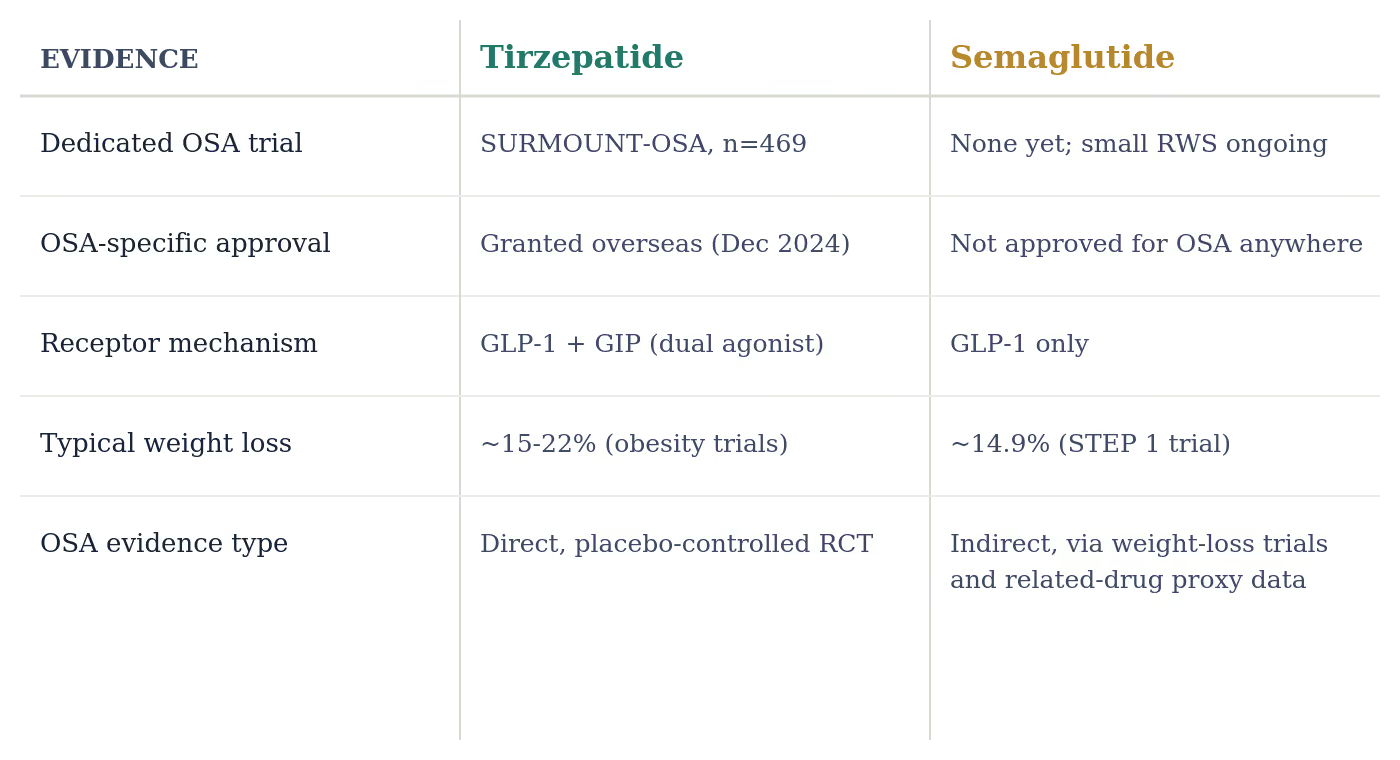
Because semaglutide is a widely used GLP-1-only weight-management injection, it's a natural point of comparison. Here's what the evidence currently shows, and doesn't show.
Semaglutide has not been evaluated in a dedicated, large-scale, placebo-controlled OSA trial in the way tirzepatide was in SURMOUNT-OSA, and it does not currently carry an approved indication for OSA in any market. (6)
The evidence for semaglutide's effect on OSA is currently indirect. In the STEP 1 trial, semaglutide produced average weight loss of 14.9% over 68 weeks versus 2.4% with placebo. Since excess weight is a primary driver of OSA severity, this degree of weight loss would be expected to meaningfully improve OSA symptoms even without a dedicated sleep apnea trial.
Small, real-world studies specifically evaluating semaglutide's effect on AHI are underway, but published results remain limited and preliminary compared with the two large, dedicated phase 3 trials behind tirzepatide's OSA data. (8) Because tirzepatide activates both the GLP-1 and GIP receptors and has shown greater weight loss than semaglutide in head-to-head comparison, some researchers propose its OSA benefit may be at least comparable. However, no trial has directly compared the two medicines specifically for sleep apnea outcomes.
在整个治疗过程中,医疗监督是必要的,以确保患者的安全和治疗的有效性。
Commonly reported effects
Studies and sources cited in this document





