









TELECONSULTATION

Enquire now



Tirzepatide is the first dual agonist weight loss injection to act on two gut hormone receptors at once, producing the largest average body-weight reductions seen in phase 3 obesity trials to date. Artisan Health Clinic offers this GLP-1 + GIP weight loss injection as part of a doctor-led weight management programme — here's what the tirzepatide injection does, what the trial data shows, and how a treatment course works here.




A note on terminology
In line with Singapore's medical advertising guidelines, this page refers to the medicine by its generic (compound) name rather than any registered trade name. Tirzepatide is available at Artisan Health Clinic, it is a prescription-only medicine, dispensed following an in-person consultation and medical assessment with one of our doctors.
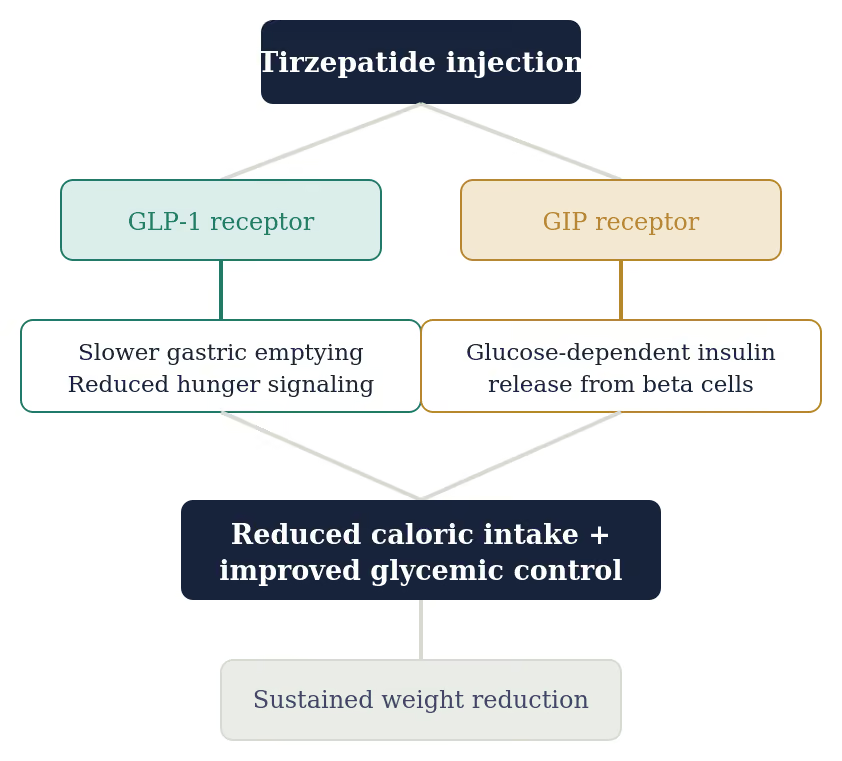
Tirzepatide is given as a once-weekly subcutaneous injection. It belongs to a class of medicines called incretin mimetics — treatments engineered to copy the action of natural gut hormones that the body releases after eating. What sets tirzepatide apart from earlier incretin-based medicines is that a single molecule is built to activate two separate hormone receptors at once: the GLP-1 receptor and the GIP receptor. This dual action is why it is described as a “dual agonist”. (2) (6).
Tirzepatide was first studied for improving blood sugar control in type 2 diabetes, then studied specifically as a weight-management treatment in adults with obesity or overweight through the SURMOUNT trial program covered later in this document.
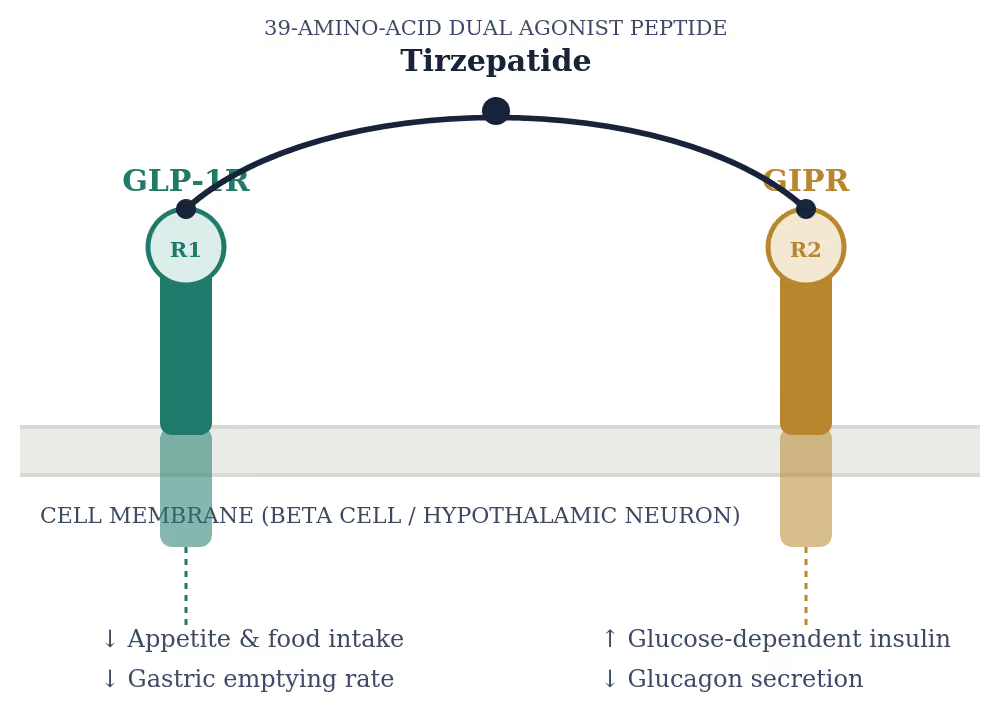
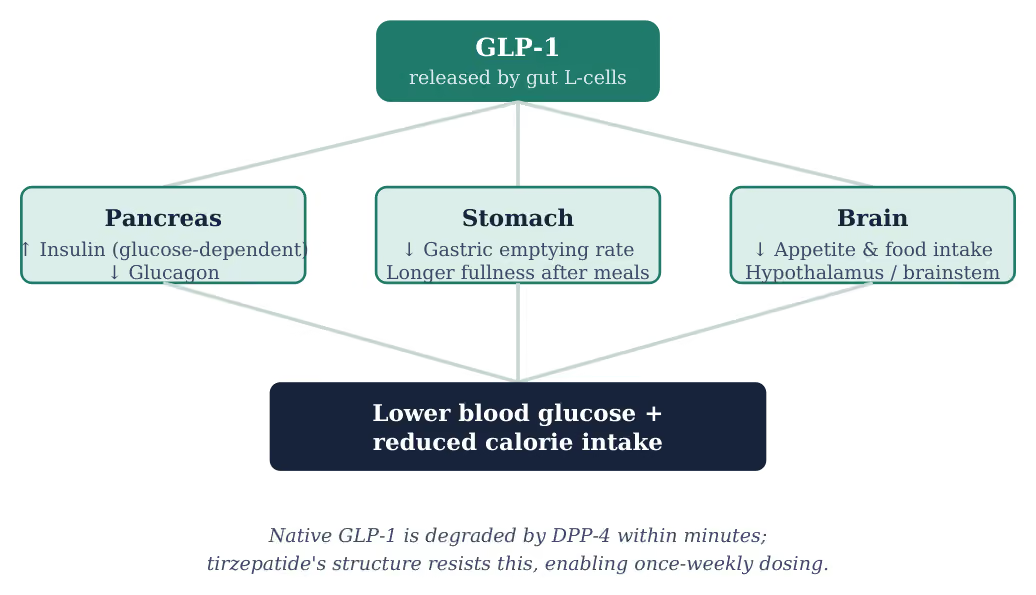
GLP-1 is a natural gut hormone released within minutes of eating. It prompts the pancreas to release insulin only when blood glucose is already elevated, while also suppressing glucagon. Together, they limit post-meal blood sugar spikes with a low risk of hypoglycemia. It also slows gastric emptying and signals directly to appetite centres in the brain, an effect now understood to be the main driver of GLP-1's impact on weight. (7) (8)Because natural GLP-1 is broken down within minutes by the enzyme DPP-4, it cannot be used as a medicine in its native form. (2)
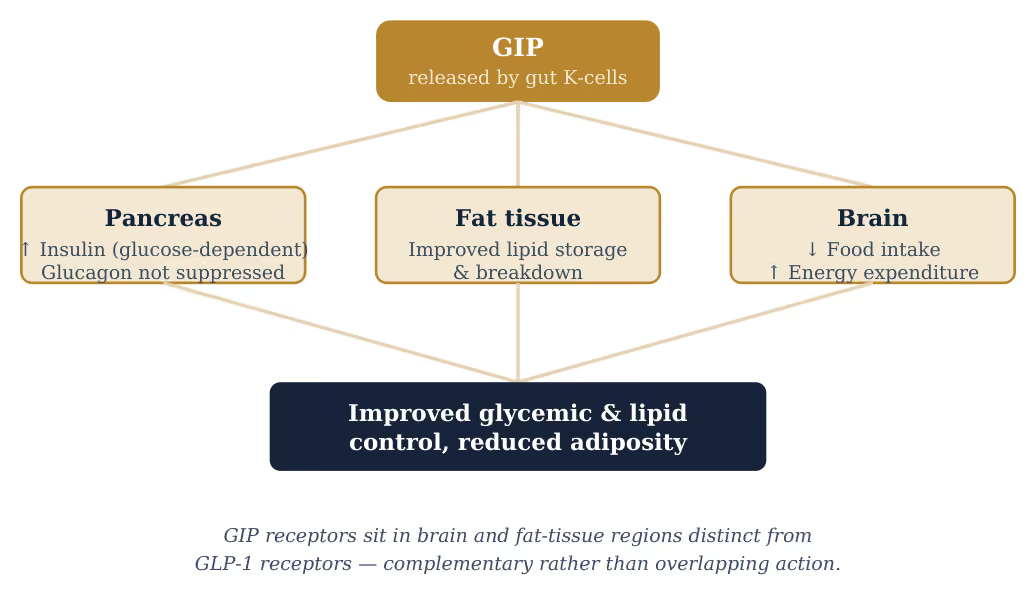
GIP was in fact the first incretin hormone identified, released from the gut in response to carbohydrate and fat intake. Like GLP-1, it stimulates glucose-dependent insulin release — but unlike GLP-1, it does not suppress glucagon, which is partly why its role in body weight was, for years, less well understood. (9)
Beyond the pancreas, GIP receptors are found in the brain and in fat tissue, where activation is linked to reduced food intake, greater energy expenditure, and improved lipid handling. (10) (11) Because GIP and GLP-1 receptors sit in overlapping but distinct locations, activating both together produces complementary effects, which is part of why dual agonism outperforms GLP-1-only treatment. (4) (10)
Structurally, tirzepatide is built on a GIP backbone with a fatty-acid side chain that binds serum albumin, extending its half-life to roughly five days. Cryo-electron microscopy and molecular dynamics work has shown that tirzepatide activates the GIP receptor in a manner nearly identical to native GIP, while engaging the GLP-1 receptor differently from native GLP-1, producing less receptor desensitization over time. (2)
Receptor-binding assays show tirzepatide is an imbalanced agonist: it engages the GIP receptor with an affinity similar to natural GIP, but binds the GLP-1 receptor roughly five-fold more weakly than native GLP-1 itself. Despite this imbalance, the combined signal from both receptors produces a stronger overall metabolic effect than maximal GLP-1 stimulation alone. (3)
In the brain, GIP receptors are expressed in overlapping but distinct regions from GLP-1 receptors, particularly in appetite-regulating areas of the hypothalamus and hindbrain. This non-identical distribution is one proposed reason dual receptor engagement produces greater appetite suppression than single-receptor agonism in preclinical models. (4)
The tirzepatide injection has been studied in a series of phase 3 randomized, double-blind, placebo-controlled trials under the SURMOUNT program. All three trials below used the same 72-week endpoint and reduced-calorie-diet-plus-exercise background, isolating the drug's effect as a dual agonist weight loss injection.
Trial
Population (n)
Result
Published
SURMOUNT-1
2,539 · obesity/overweight, no diabetes
Up to 22.5% mean weight loss (15 mg)
NEJM, 2022
SURMOUNT-2
938 · obesity/overweight + type 2 diabetes
Up to 15.7% mean weight loss (15 mg)
The Lancet, 2023
SURMOUNT-5
751 · head-to-head vs. GLP-1-only injection
Significantly greater weight loss than GLP-1-only
NEJM, 2025
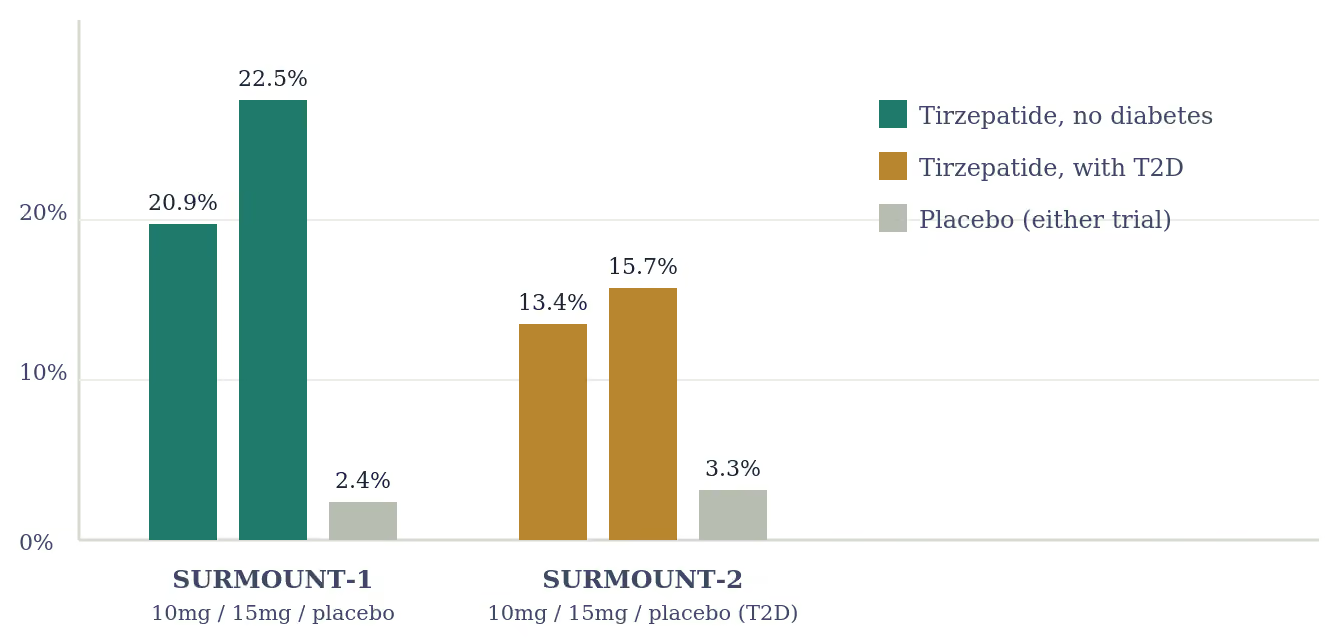
Participants without type 2 diabetes were randomized to weekly tirzepatide (5, 10, or 15 mg) or placebo for 72 weeks. Average weight reductions reached 20.9% on the 15 mg dose and 19.5% on the 10 mg dose, compared with the placebo group, with 96% of participants on the 10 mg or 15 mg dose achieving at least 5% body-weight reduction, versus 28% on placebo. (1) (3)
This trial enrolled participants with type 2 diabetes, a population that typically loses less weight on obesity drugs. Tirzepatide produced a mean weight reduction of 13.4% on the 10 mg dose and 15.7% on the 15 mg dose, versus 3.3% with placebo, with cardiometabolic markers such as triglycerides and HDL cholesterol also improving relative to placebo. (5)
The first direct comparison between a GLP-1 + GIP weight loss injection and a GLP-1-only injection. Adults with obesity or overweight and at least one weight-related condition were randomized to maximum tolerated tirzepatide (10 or 15 mg) or maximum tolerated GLP-1-only therapy weekly for 72 weeks, with tirzepatide producing significantly greater sustained weight reduction over the study period. (4)
Across the SURMOUNT program, the safety profile of this dual agonist weight loss injection has been broadly consistent with other incretin-based therapies. Most reported adverse events were gastrointestinal, generally mild to moderate, and concentrated in the dose-escalation period. (3)
Commonly reported effects
Treatment discontinuation due to adverse events occurred in roughly 3.8% of participants on the 10 mg dose and 7.4% on the 15 mg dose in SURMOUNT-2, figures broadly consistent with the SURMOUNT-1 and SURPASS diabetes trial programs. As with any incretin-based therapy, this profile reflects trial populations and may not generalize to every individual — a prescriber can assess personal risk factors, including personal or family history of medullary thyroid carcinoma.
Tirzepatide is a prescription-only medicine. It is never dispensed off-the-shelf — every course begins with an in-person medical assessment, and dosing is adjusted gradually under a doctor's supervision.




